
Your patient with chronic heart failure had a 12-Lead EKG done as part of the initial evaluation to your clinic. You note the heart rate (80 beats/minute), rhythm (regular), and intervals (all within normal limits except for a wide QRS complex (> 120 ms).
You remember the step wise process you learned for interpreting 12 Lead EKGs and check to see if there is an axis deviation. In doing so, the R axis is “normal” at -45 degrees, indicating a left axis deviation (LAD). You check for hypertrophy and note that the patient has left ventricular hypertrophy (LVH).
The question is: Does your patient have a bundle branch block?
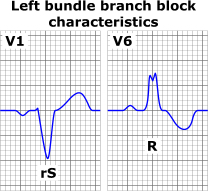
If so, it is a right bundle branch block (RBBB) or left bundle branch block (LBBB). As you look closely at the 12-leads, you remember that V1 and V6 provide the best clues in figuring this out.

After noting a wide QRS for a patient in sinus rhythm, when I am ruling out a bundle branch block, I always check for a RBBB first. It may be something to do with my love for rabbits and remembering that a RBBB looks like “rabbit ears”.
I first examine the QRS wave form in V1-V2. Normally, the QRS complex in V1 is negatively deflected. Typically, there is no Q wave since the first wave is a tiny R wave (pointing up). Most of the complex is negatively deflected (pointing downward). However, if a RBBB is present the R wave is taller (still pointing up), the S wave (more prominent) is negatively deflected (points down), and then the complex goes back up again for a taller second “R” wave. We call the second R wave “r prime” since technically the second waveform pointing up is a second R wave but we can’t call it that. Thus, the RSr’ looks like “rabbit ears”. Keep in mind that the “ears” aren’t equal in height.
I then look to V2 to see if the same rules apply, since it is the closest (contiguous) lead.
Back to my patient who has a LAD , LVH, and a wide QRS complex. It is no surprise that they did not have a RBBB. So, I move on to check for a LBBB. I focus on the lateral leads (V5-V6, I, aVL) and look for a broad or notched R wave with a prolonged upstroke in the lateral leads. It doesn’t have to be present in all four leads; likely will be in either V5-V6 or I and aVL. I also remember that ST segment depression and T wave inversion will be present. Now, being a seasoned nurse/NP in emergency and acute care settings, I have to check my own heart rate when examining an EKG with a LBBB.
At first glance, when examining a 12-Lead EKG that has a LBBB, at first glance it looks like the patient is having an acute ST-segment elevation myocardial infarction (STEMI). The wave forms in the V leads (referred to as the chest leads) jump right out at you! But remembering that the patient is stable and without symptoms, it is best to “check your excitement’ and continue with a step wise process for evaluating the EKG for a LBBB.
Normally the QRS complex in V5-V6 has a small Q wave that is negatively deflected (pointing downward), followed by a large R wave that is positively deflected (pointing upward), ending with a negatively deflected S wave. However, patients with a LBBB don’t have a Q wave (the wave form doesn’t go down first). Instead, the complex goes straight up (R wave), is notably wider than usual, and has a notch (or divot for golf enthusiasts) at the top of the complex, followed by distinct ST depression/T wave inversion. You can also check the other lateral leads (leads I and aVL) to look for a similar QRS complex. Notably, for patients with a LBBB you will see reciprocal changes in V1-V2 (it looks different but it won’t be a RBBB formation).
I hope these tips help you the next time you have a patient in sinus rhythm with a wide QRS complex. First look for those rabbit ears (albeit uneven rabbit ears); if not present then look for that what appears to be a STEMI but ends up being a LBBB.
Disclaimer: in symptomatic patients it is possible to have both (a LBBB and a STEMI), in which case you are left scratching your head, what came first, the chicken (the LBBB) or the egg (the STEMI) or did they develop simultaneously during the acute event!
Skin Bones CME Conferences
Hit the reset button while earning continuing medical education credits at our CME conferences, where you can travel to a vacation destination; earn CME credits with like-minded nurse practitioners, physician assistants, and physicians; and ‘unplug’ while enjoying a new locale! Check out our upcoming Skin, Bones, Hearts & Private Parts 2023 CME Conferences and 2024 CME Conferences! At every event, the best of the medical community gathers to earn CME credits, network, and gain knowledge on dermatology, orthopedics, cardiology and emergency medicine, women’s health, pain management and pharmacology, diabetes, ER, and mental health. On-line CME courses and Virtual CME are also available so you have the option of earning CME credits online.
See Leslie Davis speak at a 2022 Skin, Bones, Hearts & Private Parts CME Conference. Click here to find out where you can see her live and in-person!