
Abstract
Subungual hematomas can be a painful injury involving either the fingers or toes. Recognition of nailbed lacerations accompanying subungual hematomas is a diagnostic necessity. Treatment varies from simple evacuation to a complicated procedure requiring nail plate removal and laceration repair. In the case of open tuft fractures, oral antibiotics are mandatory. Long-term nail deformities are not typical, and nail regrowth can take 6 to 8 weeks.
Introduction
A subungual hematoma is an accumulation of blood between the nailbed and nail plate (finger and toe). This injury can be excruciating despite being a relatively minor injury to the finger or toe. A subungual hematoma occurring in a toe is seen commonly in runners/athletes who perform frequent cutting or sudden stop-start activities. The sudden stop-start motion causes a shearing force between the nailbed and nail plate. The shearing force results in separation of the two leading to bleeding that accumulates under the nail. Toe subungual hematomas often are associated with mal-fitting shoes and insufficient space for the toes. If there is a significant amount of blood collects under the nail, it may require drainage. These injuries involving a toe are not commonly associated with a nailbed laceration.
A crush injury to a finger can result in the formation of a subungual hematoma. Often this type of injury will increase the probability of nailbed laceration. Subungual hematomas occupying >50% of the nailbed should cause providers to be suspicious of a nailbed laceration. Providers should explore suspected nailbed injuries and repair nailbed lacerations.
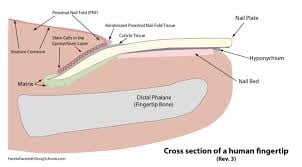
ANATOMY
Clinical Presentation
Patients with toe injuries will frequently present with pain and discoloration of the affected toenail. The amount of pain will depend on the accumulation of blood under the nail. This expanding pressure is usually the cause of the patient’s pain. In finger injuries, patients may have a disability of finger motion, sensory changes, skin trauma, and some form of nail injury. The more severe the crush injury, the more likely the patient will have more complex injuries to the finger. In that case, fractures of the distal phalanx should be considered. X-ray is an essential component in the physical examination of finger or toes crush injuries.
TREATMENT
Uncomplicated subungual hematoma
Treatment of a small (< 50%) painless subungual hematoma is usually observation only. In many cases, these small hematomas will resolve on their own without intervention. However, if blood accumulation under the nail is causing severe pain, it should be evacuated.
Providing procedural analgesia can be accomplished in a variety of maneuvers. A digital nerve block using Lidocaine or Bupivacaine offers the most complete pain relief. The quality of analgesia and duration of relief make this an easy choice. The downside is that the patient must endure an injection. For those needle-phobic patients, cryotherapy is an exciting option. Immersion of the affected digit in ice water (about 10-15 minutes) will provide adequate analgesia before trephination (decompression). Another option is to use cold spray on the finger during trephination. While cryotherapy may not offer long-duration pain relief, it does provide enough relief to allow for pressure release while improving patient comfort.
Trephination of a subungual hematoma is carried out in a variety of methods. These include thermal decompression (heated paperclip or electrocautery device) or instrumentation decompression (drill a relief hole). A hematoma occupying the entire nailbed and distending the nail plate, with proper anesthesia, can be decompressed with a scalpel blade to incise the hyponychium skin. This will evacuate the hematoma without damage to the nail plate.
A loose compressive bandage is used to keep the drill hole(s) patent and allow for fluid drainage. Daily warm soapy water soaks (10-15min) will keep the wounds clean and nail plate openings patent. Post-procedural pain management following trephination involves Acetaminophen, NSAIDs, or Cryotherapy. In most cases, the affected nail plate will fall off. Growth of a new nail can occur in 6-8 weeks and usually results in a regular appearing nail. There is always a chance that the germinal matrix was injured, leading to a deformity as the new nail regrows.
Crush-injury/Nail bed Laceration/Tuft fracture
Crush injuries to the distal phalanx can result in a tuft fracture with or without a nail bed laceration. X-ray evaluation revealing a Tuft fracture (fracture of the distal phalanx) and in the presence of subungual hematoma (>50%) would indicate an open fracture. If this occurs then, the nail plate should be removed, and the underlying skin laceration repaired. The nail should be saved and loosely sutured over the nailbed laceration to protect the healing skin. Patients should be started on oral antibiotic coverage for 7-10 days. Follow-up should be arranged within 3-5 days for open fractures is recommended. Post-procedural pain management following trephination, nail-plate removal, and/or laceration repair can involve a combination of NSAIDS, Cryotherapy, and narcotic analgesics. Growth of a new nail can occur in 6-8 weeks and usually results in a regular-looking nail. However, there is always a chance that the new nail-plate will have some deformity as it regrows.
Conclusion
Subungual hematomas can be a painful injury involving either the fingers or toes. Recognition of nailbed lacerations that can accompany subungual hematomas is a diagnostic necessity. Treatment varies from simple evacuation to a complicated procedure that requires nail-plate removal and laceration repair. In the case of open tuft fractures, oral antibiotics are mandatory. Long-term nail deformities are not typical, and nail regrowth can take 6 to 8 weeks.
See Tom Gocke, DMSc, ATC, PA-C, DFAAPA speak at a 2021 Skin, Bones, Hearts & Private Parts CME Conference in Destin, Myrtle Beach, Chicago , Orlando, or Las Vegas.
In-person, Live Stream, or On-demand