Atrial Fibrillation
Atrial fibrillation (AF) is a common supraventricular arrhythmia that increases in prevalence with age and significantly increases the risk of embolic stroke. Therefore, healthcare providers need to know current treatment options to prevent cardiovascular sequela associated with AF. But, first, the practicing clinician must identify AF, perform the essential diagnostic evaluation, and perform a stroke risk assessment. Then, develop a shared decision-making plan for potential anticoagulation to reduce thromboembolism risk. The American College of Cardiology/American Heart Association/Heart Rhythm Society Atrial Fibrillation Guidelines emphasize practical approaches and clinical pearls to translate scientific evidence into everyday practice. Also, provide a framework for clinicians to reduce stroke risk associated with AF and improve patient outcomes.

Case Study
Let’s review the case of Mr. Skip A. Beat, a 70-year-old Caucasian male who presents to the outpatient cardiology clinic for palpitations. He has a past medical history of hypertension, diabetes mellitus type 2, dyslipidemia, and obesity.
Mr. Skip A. Beat reports that his “heart is jumping all over the place .”He has mild shortness of breath with moderate exertional activities such as walking uphill or climbing one flight of stairs. He denies orthopnea, paroxysmal nocturnal dyspnea, or lower extremity edema. He denies chest pain, pressure, or tightness.
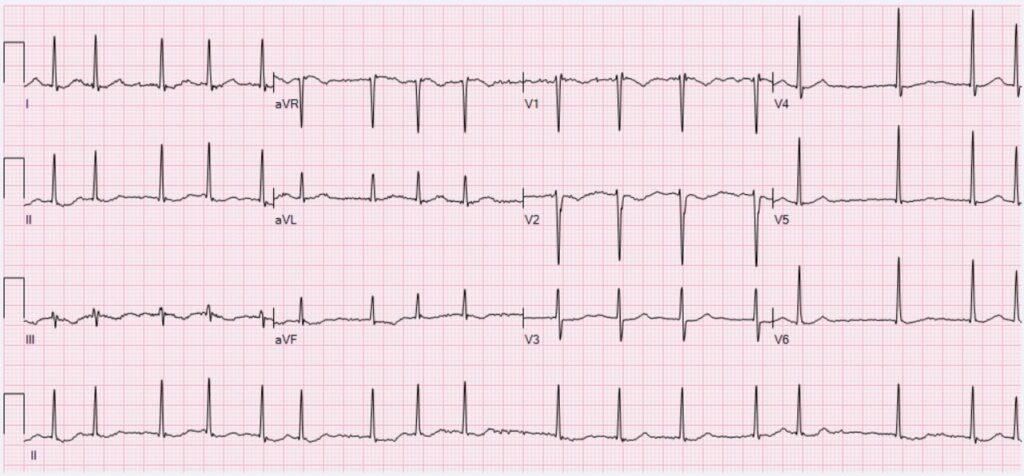
His blood pressure is 128/70, pulse 98, respiratory rate of 18, and Sp02 of 98%. He is in no acute distress on physical exam, speaking in complete unlabored sentences. His jugular venous pressure is 8cm of H20, breath sounds are clear to auscultation, heart rhythm is irregularly irregular, with S1 and S2 sounds, and no murmurs, gallops, or rubs noted. His laboratory tests (basic metabolic panel, lipid panel, BNP, CBC, TSH) were unremarkable and ordinary. His ECG shows atrial fibrillation. His echocardiogram resulted in an ejection fraction of 55% with no valvular heart disease.
What are the next steps?
What are the next steps in the management of confirmed atrial fibrillation? Given that Mr. Skip A. Beat has a confirmed diagnosis of AF, a stroke risk assessment should perform using a stroke risk calculator such as the CHA2DS2-Vasc calculator. The CHA2DS2-Vasc calculator is at AnticoagEvaluator (acc.org). Based on his demographic information and medical history, Mr. Skip A. Beat’s CHA2DS2-Vasc score is 3, which means he has a 3.2% adjusted annual risk of stroke with no therapy.
After a decision-making discussion, Mr. Skip A. Beat decided to start a non–vitamin K oral anticoagulant (NOAC). That can reduce his annual risk of stroke and thromboembolism to 1.1%. He will have a follow-up appointment in the cardiology clinic in one month to discuss strategies to restore sinus rhythm. In addition, he is sent for a sleep apnea study and counseled to avoid alcohol intake, both risk factors for AF development.
Management of HFrEF requires timely initiation and up-titration of GDMT and is proven to reduce morbidity and mortality with benefits seen within the first 30 days of initiation. Therapeutic benefits are seen early after initiation of GDMT, so avoid therapeutic inertia in your clinical practice and start your patients with HFrEF on these life-saving medications early and up-titrate to doses where the most benefit was found in clinical trials.
Skin Bones CME Conferences
Hit the reset button while earning continuing medical education credits at our CME conferences, where you can travel to a vacation destination; earn CME credits with like-minded nurse practitioners, physician assistants, and physicians; and ‘unplug’ while enjoying a new locale! Check out our upcoming Skin, Bones, Hearts & Private Parts 2023 CME Conferences and 2024 CME Conferences! At every event, the best of the medical community gathers to earn CME credits, network, and gain knowledge on dermatology, orthopedics, cardiology and emergency medicine, women’s health, pain management and pharmacology, diabetes, ER, and mental health. On-line CME courses and Virtual CME are also available so you have the option of earning CME credits online.
References:
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons [published correction appears in Circulation. 2019 Aug 6;140(6):e285]. Circulation. 2019;140(2):e125-e151. doi:10.1161/CIR.0000000000000665
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2014 Dec 2;64(21):2305-7]. J Am Coll Cardiol. 2014;64(21):e1-e76. doi:10.1016/j.jacc.2014.03.022